The blog will contain brief summaries of recent publications relevant to obstetric anaesthesia.
Views posted are those of the author (E Plunkett, unless specified). If you would like to contribute please contact us.
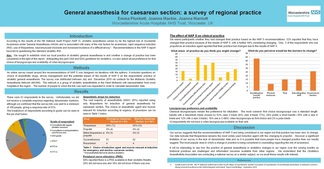
General anaesthesia (GA) for Caesarean Section (CS) in the West Midlands: have we changed our practice since the publication of NAP 5?
Last year we sent a survey out through our network contacts, to ask about individual's practice of GA CS, particularly with respect to choice of induction agent and whether practice had changed since the results of NAP 5. A summary of the results was presented as a poster at the OAA and a copy of this can be downloaded here, but of note, thiopentone remains the most commonly used induction agent in our region.
There were several other posters on the same theme, and all the posters can be viewed online here. Posters on a similar subject are:
Last year we sent a survey out through our network contacts, to ask about individual's practice of GA CS, particularly with respect to choice of induction agent and whether practice had changed since the results of NAP 5. A summary of the results was presented as a poster at the OAA and a copy of this can be downloaded here, but of note, thiopentone remains the most commonly used induction agent in our region.
There were several other posters on the same theme, and all the posters can be viewed online here. Posters on a similar subject are:
- P60 is the OAA approved impact of NAP5 survey results, which shows that the use of propofol is increasing but it is still used by only 27% of respondents.
- P92 gives the Irish perspective, which suggests that change is slow to occur in Ireland too.
- P57 is a regional survey of practice in the Severn region where they now more commonly (68%) use propofol.
- P35 and P121 look at the effect of using propofol on maternal and fetal outcomes. The former found a reduction in maternal hypertension on intubation but increased used of vasopressors and an increase in difficult intubation with propofol, but no adverse effects on neonates. The latter found no evidence of worsened maternal or fetal outcomes.

April 15: Measuring block height Anaesthesia 2015, 70, 421-428
In the April Edition of Anaesthesia there was an article by Hoyle and Yentis on the subject of how we assess the height of the block (epidural or spinal) before caesarean section (CS). We all have our own way of assessing block height and surveys would suggest there is some variation, although assessment to cold is most frequent. The authors point out that basing one’s practice on the results of surveys is potentially flawed: surveys (if the response rate is sufficient for them to be considered representative) tell us what current practice is, rather than what it should be. This study looked at the method of assessment of block height in an impressive 284 papers and 45 editions of anaesthetic textbooks. The bottom line from the results is that there is still wide variation although, for spinals at least, there is an increasing trend towards assessing light touch to T5 and T6. For epidurals T4 was more common. In only 4/284 of the papers was the level correlated with a dermatome map or surface anatomy and only 40% documented motor block, mostly using the Bromage score.
This study raises the question of whether we need a scoring system for assessing the block level before CS. Pain during CS remains a significant cause of litigation and confusion over which method to use to assess the block, may lead to difficulty in working out whether the patient has been managed appropriately. This uncertainty also extends into the world of research as it makes it harder to compare techniques or drugs. One trend that the authors note, which I have also observed in practice, is that people often use several methods of assessment of block height. This can be reassuring if all methods give consistent results and if this is not the case, may help us counsel our patients accordingly. The final word has to be that documentation is key - of block height (however it is measured), of any discussion with patient and of the agreed plan that results from this.
In the April Edition of Anaesthesia there was an article by Hoyle and Yentis on the subject of how we assess the height of the block (epidural or spinal) before caesarean section (CS). We all have our own way of assessing block height and surveys would suggest there is some variation, although assessment to cold is most frequent. The authors point out that basing one’s practice on the results of surveys is potentially flawed: surveys (if the response rate is sufficient for them to be considered representative) tell us what current practice is, rather than what it should be. This study looked at the method of assessment of block height in an impressive 284 papers and 45 editions of anaesthetic textbooks. The bottom line from the results is that there is still wide variation although, for spinals at least, there is an increasing trend towards assessing light touch to T5 and T6. For epidurals T4 was more common. In only 4/284 of the papers was the level correlated with a dermatome map or surface anatomy and only 40% documented motor block, mostly using the Bromage score.
This study raises the question of whether we need a scoring system for assessing the block level before CS. Pain during CS remains a significant cause of litigation and confusion over which method to use to assess the block, may lead to difficulty in working out whether the patient has been managed appropriately. This uncertainty also extends into the world of research as it makes it harder to compare techniques or drugs. One trend that the authors note, which I have also observed in practice, is that people often use several methods of assessment of block height. This can be reassuring if all methods give consistent results and if this is not the case, may help us counsel our patients accordingly. The final word has to be that documentation is key - of block height (however it is measured), of any discussion with patient and of the agreed plan that results from this.
Dec 2014 Saving Lives: Improving Mothers' Care
The latest confidential enquiry into Maternal Deaths was published in December. The structure of the reports has changed slightly and it now includes maternal deaths in Ireland and also reviews the care of women with severe complications in pregnancy, who survived.
357 women died during pregnancy or within 6 weeks of delivery in this triennium (2009-12). The mortality rate has decreased significantly to 10.12 per 100,000 pregnancies. Only one third of these deaths were from direct causes, and almost three quarters of those who died had a pre-existing medical condition. Almost a quarter died from sepsis and 1 in 11 of the deaths were from influenza.
This report includes reviews of the following topics: sepsis; haemorrhage; amniotic fluid embolism
anaesthesia-related causes; neurological causes; other indirect causes. Each of these topics will be included once every 3 years and other topics will be covered in annual reports in the years in between.
Key messages for anaesthesia are:
To download the report please click here.
The latest confidential enquiry into Maternal Deaths was published in December. The structure of the reports has changed slightly and it now includes maternal deaths in Ireland and also reviews the care of women with severe complications in pregnancy, who survived.
357 women died during pregnancy or within 6 weeks of delivery in this triennium (2009-12). The mortality rate has decreased significantly to 10.12 per 100,000 pregnancies. Only one third of these deaths were from direct causes, and almost three quarters of those who died had a pre-existing medical condition. Almost a quarter died from sepsis and 1 in 11 of the deaths were from influenza.
This report includes reviews of the following topics: sepsis; haemorrhage; amniotic fluid embolism
anaesthesia-related causes; neurological causes; other indirect causes. Each of these topics will be included once every 3 years and other topics will be covered in annual reports in the years in between.
Key messages for anaesthesia are:
- Consider subdural haematoma and cerebral venous sinus thrombosis in the differential diagnosis for PDPH
- Anaesthetists should practice drills for managing peri-operative airway emergencies
- Pregnant or post-partum women need the same standards of post-operative monitoring as non-obstetric patients
- Anaesthetists should be ready to deal with side effects of local anaesthetics and minimise the use of higher concentrations
- Prompt action and effective communication is essential for managing sudden unexpected catastrophes
- Ambulance staff should be trained to relieve aortocaval compression and should document how this is done
- Units should ensure women are appropriately monitored
- All SUI investigations should include an obstetric anaesthetist.
To download the report please click here.
Oct 2014: BJA and Anaesthesia
September this year saw the publication of the results of NAP5 - the largest ever study of Accidental Awareness under General Anaesthesia (AAGA) in the world. In the October editions of the BJA and Anaesthesia there are various editorials and original articles discussing this report. Its unique methodology, assessing the number of spontaneously recorded cases in a 12 month period, yielded a lower incidence of AAGA than previous studies, with the overall incidence of AAGA from NAP5 is 1:19600.
Many risk factors were identified. Notably for obstetric anaesthesia, these include being young, female, obese, and having a difficult airway. Anaesthetic risk factors include thiopentone, RSI and use of NMB as mentioned above. Obstetric cases represented 10% of the cases of AAGA but only 0.8% of the cases in the activity survey making it the most over-represented specialty.
The incidence of AAGA in obstetrics from this study ranges from 1:670 - 920 (denominator data dependent), which is much closer to the previously reported incidences from studies using the Brice questionnaire to identify cases. It has been postulated that this is due to the rigorous follow up that occurs after anaesthetic intervention in obstetrics and this certainly seems plausible.
So what do we do with this information? The recommendations specific to obstetric anaesthesia in the study are:
1. Communicating the high risk for AAGA appropriately to patients as part of the consent process
2. Attempts to reduce the risk of AAGA by ensuring adequate doses of anaesthetic agent (both IV and inhalational)
3. Planning for management of the difficult airway with consideration to making a second syringe of IV agent available
4. Consideration of failed regional anaesthesia as an additional risk factor for AAGA
5. Being mindful that antibiotic syringes are a latent risk for drug error and attempts should be made to mitigate this by adapting systems accordingly. For example, consider allocating the task of antibiotics administration to non anaesthetists
These recommendations seem reasonable, with possibly the most challenging being appropriate and timely consent of patients, an area which is already considered difficult in obstetrics at times. Indeed, many of the messages that we as individuals can take from NAP 5 are related to communication with patients. If we let patients know what to expect (for example that they might recall extubation if this is planned to be awake); if we consent them appropriately; if we speak to reassure them if AAGA is suspected intra-operatively and if we can take any reports of AAGA seriously and act quickly, we can reduce the harm caused by any recall that is experienced. Combine this with attention to detail during the case, timely communication with the theatre team and steps to mitigate latent risks and we will be doing all we can to prevent awareness occurring. The report is lengthy, but well worth a read, as are the associated articles and editorials. http://nap5.org.uk/NAP5report
September this year saw the publication of the results of NAP5 - the largest ever study of Accidental Awareness under General Anaesthesia (AAGA) in the world. In the October editions of the BJA and Anaesthesia there are various editorials and original articles discussing this report. Its unique methodology, assessing the number of spontaneously recorded cases in a 12 month period, yielded a lower incidence of AAGA than previous studies, with the overall incidence of AAGA from NAP5 is 1:19600.
Many risk factors were identified. Notably for obstetric anaesthesia, these include being young, female, obese, and having a difficult airway. Anaesthetic risk factors include thiopentone, RSI and use of NMB as mentioned above. Obstetric cases represented 10% of the cases of AAGA but only 0.8% of the cases in the activity survey making it the most over-represented specialty.
The incidence of AAGA in obstetrics from this study ranges from 1:670 - 920 (denominator data dependent), which is much closer to the previously reported incidences from studies using the Brice questionnaire to identify cases. It has been postulated that this is due to the rigorous follow up that occurs after anaesthetic intervention in obstetrics and this certainly seems plausible.
So what do we do with this information? The recommendations specific to obstetric anaesthesia in the study are:
1. Communicating the high risk for AAGA appropriately to patients as part of the consent process
2. Attempts to reduce the risk of AAGA by ensuring adequate doses of anaesthetic agent (both IV and inhalational)
3. Planning for management of the difficult airway with consideration to making a second syringe of IV agent available
4. Consideration of failed regional anaesthesia as an additional risk factor for AAGA
5. Being mindful that antibiotic syringes are a latent risk for drug error and attempts should be made to mitigate this by adapting systems accordingly. For example, consider allocating the task of antibiotics administration to non anaesthetists
These recommendations seem reasonable, with possibly the most challenging being appropriate and timely consent of patients, an area which is already considered difficult in obstetrics at times. Indeed, many of the messages that we as individuals can take from NAP 5 are related to communication with patients. If we let patients know what to expect (for example that they might recall extubation if this is planned to be awake); if we consent them appropriately; if we speak to reassure them if AAGA is suspected intra-operatively and if we can take any reports of AAGA seriously and act quickly, we can reduce the harm caused by any recall that is experienced. Combine this with attention to detail during the case, timely communication with the theatre team and steps to mitigate latent risks and we will be doing all we can to prevent awareness occurring. The report is lengthy, but well worth a read, as are the associated articles and editorials. http://nap5.org.uk/NAP5report

Aug 2014: IJOA Volume 23 Issue 3 P 201-203 & P206-212
How good are we at predicting the vertebral interspace at which we insert our spinal needles? In this issue of IJOA there is an editorial and an original article on this subject. The editorial by Dr Bogod quotes a previous editorial by Dr Reynolds in 2000, stating, “The L2-3 interspace should not be an option, and several textbooks need to be rewritten to account for human variability”. Dr Reynolds editorial was prompted by a study in the same journal which revealed that the anaesthestist predicted the correct interspace in only 29% of cases and that the vast majority of incorrect predications were too low. This was felt to be related to the fact that interpretation of Tuffier’s line for surface anatomy is not as straightforward as radiologically – hence the reference to rewriting textbooks. Indeed, other studies have shown that the line intersects the midline at or above L2-3 in up to 51% of patients. As we all know, the consequences of too high an insertion point can be catastrophic for the patient and Dr Bogod reminds us of the medico-legal implications too.
So how can we minimise the chances of error? The original article by K K Srinivasan et al from Dublin compared 2 landmark techniques for identifying a safe space for spinal needle insertion, the aim being to develop a safe protocol. The authors recruited 110 patients having elective caesarean section under spinal anaesthesia and randomised them to one of 2 groups. In Group A, if Tuffier's line (the intercristal line) intersected an intervertebral space, this space was selected. If it intersected a spinous process the space above was selected. In Group B, whether the intercristal line intersected a spinous process or a space, the space below was selected. The position that had been selected was then verified by a blinded, experienced (> 75 neuraxial ultrasound examinations previously) investigator, with the primary endpoint of the study being the proportion of interspaces marked at or above L2-3. Unsurprisingly this was significantly higher in Group A, with 45.5% of cases being at L2-3 or higher, compared with 7.3% in Group B. Furthermore 9.1% of patients in Group A had the L1-2 interspace marked compared with none in Group B. Interestingly, in only 20% of cases was the palpated intercristal line at the spinous process of L4 or below. The authors reported no difference in difficulties with insertion of the spinal (they did not allow insertion to be attempted at L1-2), effectiveness of the block or complications.
There are obvious limitations to this study: ultrasound identification of anatomy is not infallible, the experience of the anaesthetists varied and patients in whom the spinous processes or intervertebral spaces could not be palpated were excluded. However, the underlying message, that we often insert our spinal needle higher than we think, is cautionary and worth remembering. As the authors suggest: whatever is palpated in the intercristal line, choose a space below and this should minimise the chances of insertion at L2-3 (or higher).
How good are we at predicting the vertebral interspace at which we insert our spinal needles? In this issue of IJOA there is an editorial and an original article on this subject. The editorial by Dr Bogod quotes a previous editorial by Dr Reynolds in 2000, stating, “The L2-3 interspace should not be an option, and several textbooks need to be rewritten to account for human variability”. Dr Reynolds editorial was prompted by a study in the same journal which revealed that the anaesthestist predicted the correct interspace in only 29% of cases and that the vast majority of incorrect predications were too low. This was felt to be related to the fact that interpretation of Tuffier’s line for surface anatomy is not as straightforward as radiologically – hence the reference to rewriting textbooks. Indeed, other studies have shown that the line intersects the midline at or above L2-3 in up to 51% of patients. As we all know, the consequences of too high an insertion point can be catastrophic for the patient and Dr Bogod reminds us of the medico-legal implications too.
So how can we minimise the chances of error? The original article by K K Srinivasan et al from Dublin compared 2 landmark techniques for identifying a safe space for spinal needle insertion, the aim being to develop a safe protocol. The authors recruited 110 patients having elective caesarean section under spinal anaesthesia and randomised them to one of 2 groups. In Group A, if Tuffier's line (the intercristal line) intersected an intervertebral space, this space was selected. If it intersected a spinous process the space above was selected. In Group B, whether the intercristal line intersected a spinous process or a space, the space below was selected. The position that had been selected was then verified by a blinded, experienced (> 75 neuraxial ultrasound examinations previously) investigator, with the primary endpoint of the study being the proportion of interspaces marked at or above L2-3. Unsurprisingly this was significantly higher in Group A, with 45.5% of cases being at L2-3 or higher, compared with 7.3% in Group B. Furthermore 9.1% of patients in Group A had the L1-2 interspace marked compared with none in Group B. Interestingly, in only 20% of cases was the palpated intercristal line at the spinous process of L4 or below. The authors reported no difference in difficulties with insertion of the spinal (they did not allow insertion to be attempted at L1-2), effectiveness of the block or complications.
There are obvious limitations to this study: ultrasound identification of anatomy is not infallible, the experience of the anaesthetists varied and patients in whom the spinous processes or intervertebral spaces could not be palpated were excluded. However, the underlying message, that we often insert our spinal needle higher than we think, is cautionary and worth remembering. As the authors suggest: whatever is palpated in the intercristal line, choose a space below and this should minimise the chances of insertion at L2-3 (or higher).

Aug 2014: IJOA Volume 23 Issue 3 P 213-216
The use of ultrasound to identify the correct space is worthy of discussion and remains controversial. Whilst there is undoubtably a learning curve to this, the study described above might lead one to conclude that we should be using ultrasound regularly to improve accuracy of identification of intervertebral space and thus to increase safety. Those in favour of ultrasound may argue that it also improves success rate, whereas those against may state that it takes too long. Another original article in the same issue of IJOA by Ansari et al sought to answer these questions. They randomised 150 women to have insertion of spinal anaesthesia guided by ultrasound or landmark technique (which involved palpation of Tuffier’s line to identify the L3-4 or L4-5 interspace, which we now know may lead to inaccuracy). They found no difference in the average procedure time, number of skin punctures or needle passes, or success rates.
So should we be using ultrasound or not? The result of the study by Srinivasan et al would suggest that, as long as care is taken to choose a space below the intercristal line for insertion of our needles, then we should be safe without it. However, the argument that we need to learn to help with difficult cases is valid and the study by Ansari et al would suggest that in the hands of an experienced anaesthetist, it does not add to the procedure time significantly.
The use of ultrasound to identify the correct space is worthy of discussion and remains controversial. Whilst there is undoubtably a learning curve to this, the study described above might lead one to conclude that we should be using ultrasound regularly to improve accuracy of identification of intervertebral space and thus to increase safety. Those in favour of ultrasound may argue that it also improves success rate, whereas those against may state that it takes too long. Another original article in the same issue of IJOA by Ansari et al sought to answer these questions. They randomised 150 women to have insertion of spinal anaesthesia guided by ultrasound or landmark technique (which involved palpation of Tuffier’s line to identify the L3-4 or L4-5 interspace, which we now know may lead to inaccuracy). They found no difference in the average procedure time, number of skin punctures or needle passes, or success rates.
So should we be using ultrasound or not? The result of the study by Srinivasan et al would suggest that, as long as care is taken to choose a space below the intercristal line for insertion of our needles, then we should be safe without it. However, the argument that we need to learn to help with difficult cases is valid and the study by Ansari et al would suggest that in the hands of an experienced anaesthetist, it does not add to the procedure time significantly.
July 2014 : Anaesthesia Vol 69 No 7
The editorial by Dr Palanisamy (Boston) and Dr Bailey (London) entitled "Codeine in mothers and children: where are we now?" was prompted by the tragic death of a toddler in the USA following use of codeine as post tonsillectomy analgesia. Their article calls into question the use of codeine as an analgesic after decades of what has thought to be safe use worldwide. In the editorial the authors first remind us that genetic polymorphisms lead to significant differences in the metabolism of codeine to morphine between individuals and a wide variation in its effectiveness. They also question whether codeine is really safe to use in pregnancy, citing conflicting evidence of its association with congenital abnormalities. They go on to discuss whether use of codeine in pregnancy is associated with adverse obstetric outcomes, concluding that further evaluation is needed.
The use of codeine as a post partum analgesic is then addressed. It is known to be secreted in breast milk (albeit in small quantities) and may lead to CNS depression, especially if the mother is an ultra metaboliser (via high levels of morphine). Moreover it has been shown that it is less effective than NSAIDs with a worse side effect profile. They conclude that one approach would be to avoid it in ethnicities at risk of being ultra metabolisers (Ethopians for example) and limit the dose in others to 1mg/kg/day. However, as they say, it may be better to avoid it altogether.
Are we still using codeine and is it really justified?
The editorial by Dr Palanisamy (Boston) and Dr Bailey (London) entitled "Codeine in mothers and children: where are we now?" was prompted by the tragic death of a toddler in the USA following use of codeine as post tonsillectomy analgesia. Their article calls into question the use of codeine as an analgesic after decades of what has thought to be safe use worldwide. In the editorial the authors first remind us that genetic polymorphisms lead to significant differences in the metabolism of codeine to morphine between individuals and a wide variation in its effectiveness. They also question whether codeine is really safe to use in pregnancy, citing conflicting evidence of its association with congenital abnormalities. They go on to discuss whether use of codeine in pregnancy is associated with adverse obstetric outcomes, concluding that further evaluation is needed.
The use of codeine as a post partum analgesic is then addressed. It is known to be secreted in breast milk (albeit in small quantities) and may lead to CNS depression, especially if the mother is an ultra metaboliser (via high levels of morphine). Moreover it has been shown that it is less effective than NSAIDs with a worse side effect profile. They conclude that one approach would be to avoid it in ethnicities at risk of being ultra metabolisers (Ethopians for example) and limit the dose in others to 1mg/kg/day. However, as they say, it may be better to avoid it altogether.
Are we still using codeine and is it really justified?
July 2014 : Anaesthesia Vol 69 No 7
The results of an OAA sponsored survey on the use of obstetric early warning systems are reported later in the journal. Of the 130/205 (63%) lead Anaesthetists who responded to the survey, all were using systems, up from only 19% in 2007. The article reiterates that scoring systems are recommended by NICE and other national guidance such as that from the Confidential Enquiry into Maternal Deaths (CEMD) which recommended the modified early obstetric warning system (MEOWS). Indeed 45% of units responding used this chart with 50% using a modified version and 5% a different system. There was good agreement amongst respondents on the important variables to measure. Predictably, the reported barriers to implementation were staffing pressures and lack of teaching but despite these difficulties 91% of those responding felt that the scoring system was a useful tool to aid with reduction of maternal morbidity.
The results of an OAA sponsored survey on the use of obstetric early warning systems are reported later in the journal. Of the 130/205 (63%) lead Anaesthetists who responded to the survey, all were using systems, up from only 19% in 2007. The article reiterates that scoring systems are recommended by NICE and other national guidance such as that from the Confidential Enquiry into Maternal Deaths (CEMD) which recommended the modified early obstetric warning system (MEOWS). Indeed 45% of units responding used this chart with 50% using a modified version and 5% a different system. There was good agreement amongst respondents on the important variables to measure. Predictably, the reported barriers to implementation were staffing pressures and lack of teaching but despite these difficulties 91% of those responding felt that the scoring system was a useful tool to aid with reduction of maternal morbidity.
